From
WIKIPEDIA
: This copy-pasted Wikipedia
webpage was last modified on 17 July 2010 at 01:39.
Jump to: a href="#mw-head">navigation,
search
Malaria is a
mosquito-borne
infectious disease caused by a
eukaryotic
protist of the genus
Plasmodium. It is widespread in
tropical and subtropical regions, including parts of the
Americas (22 countries),
Asia,
and
Africa. Each year, there are approximately 350–500 million cases
of malaria,[1]
killing between one and three million people, the majority of whom
are young children in
sub-Saharan Africa.[2]
Ninety percent of malaria-related deaths occur in sub-Saharan
Africa. Malaria is commonly associated with poverty, but is also a
cause of poverty[3]
and a major hindrance to
economic development.
Five species of the plasmodium parasite can infect humans; the
most serious forms of the disease are caused by
Plasmodium falciparum. Malaria caused by
Plasmodium vivax,
Plasmodium ovale and
Plasmodium malariae causes milder disease in humans that is
not generally fatal. A fifth species,
Plasmodium knowlesi, is a
zoonosis that causes malaria in
macaques but can also infect humans.[4][5]
Malaria is naturally transmitted by the bite of a female
Anopheles mosquito. When a mosquito bites an infected
person, a small amount of blood is taken, which contains malaria
parasites. These develop within the mosquito, and about one week
later, when the mosquito takes its next blood meal, the parasites
are injected with the mosquito's saliva into the person being
bitten. After a period of between two weeks and several months
(occasionally years) spent in the liver, the malaria parasites start
to multiply within
red blood cells, causing symptoms that include
fever,
and
headache. In severe cases the disease worsens leading to
hallucinations,
coma,
and death.
A wide variety of
antimalarial drugs are available to treat malaria. In the last 5
years, treatment of P. falciparum infections in
endemic countries has been transformed by the use of
combinations of drugs containing an
artemisinin derivative. Severe malaria is treated with
intravenous or intramuscular quinine or, increasingly, the
artemisinin derivative artesunate.[6]
Several drugs are also available to prevent malaria in travellers to
malaria-endemic
countries (prophylaxis).
Resistance has developed to several antimalarial drugs, most notably
chloroquin
7]
Malaria transmission can be reduced by preventing mosquito bites
by distribution of inexpensive
mosquito nets and
insect repellents, or by mosquito-control measures such as
spraying
insecticides inside houses and draining standing water where
mosquitoes lay their eggs.
Although many are under development, the challenge of producing a
widely available
vaccine that provides a high level of protection for a sustained
period is still to be met.[8]
[edit]
Signs and symptoms
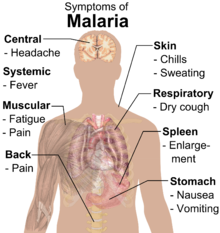
Main symptoms of malaria.
[9]

Typical fever patterns in Malaria.
Symptoms of malaria include
fever,
shivering,
arthralgia (joint pain),
vomiting,
anemia
(caused by
hemolysis),
hemoglobinuria,
retinal damage,[10]
and
convulsions. T
The classic symptom of malaria is cyclical
occurrence of sudden coldness followed by
rigor and then fever and sweating lasting four to six hours,
occurring every two days in P. vivax and P. ovale
infections, while every three days for P. malariae.[11]
P. falciparum can have recurrent fever every 36–48 hours or a
less pronounced and almost continuous fever.
For reasons that are
poorly understood, but that may be related to high
intracranial pressure, children with malaria frequently exhibit
abnormal posturing, a sign indicating severe brain damage.[12]
Malaria has been found to cause cognitive impairments, especially in
children. It causes widespread
anemia
during a period of rapid brain development and also direct brain
damage. This neurologic damage results from cerebral malaria to
which children are more vulnerable.[13][14]
Cerebral malaria is associated with retinal whitening,[15]
which may be a useful clinical sign in distinguishing malaria from
other causes of fever.[16]
SeSevere malaria is almost exclusively caused by P. falciparum
infection, and usually arises 6–14 days after infection.[17]
Consequences of severe malaria include
coma
and death if untreated—young children and pregnant women are
especially vulnerable.
Splenomegaly (enlarged spleen), severe
headache, cerebral
ischemia,
hepatomegaly (enlarged liver),
hypoglycemia, and hemoglobinuria with
renal failure may occur.
Renal failure may cause
blackwater fever, where hemoglobin from lysed red blood cells
leaks into the urine. Severe malaria can progress extremely rapidly
and cause death within hours or days.[span>17]
In the most severe cases of the disease, fatality rates can exceed
20%, even with intensive care and treatment.[18]
In endemic areas, treatment is often less satisfactory and the
overall fatality rate for all cases of malaria can be as high as one
in ten.[19]
Over the longer term, developmental impairments have been documented
in children who have suffered episodes of severe malaria.[20]
Chronic malaria is seen in both P. vivax and P. ovale,
but not in P. falciparum. Here, the disease can relapse
months or years after exposure, due to the presence of latent
parasites in the liver. Describing a case of malaria as cured by
observing the disappearance of parasites from the bloodstream can,
therefore, be deceptive. The longest incubation period reported for
a P. vivax infection is 30 years.[17]
Approximately one in five of P. vivax malaria cases in
temperate areas involve
overwintering by hypnozoites (i.e., relapses begin the year
after the mosquito bite).[span>21]
[edit]
Causes

A
Plasmodium sporozoite traverses the cytoplasm
of a mosquito midgut epithelial cell in this false-color
electron micrograph.
[edit]
Malaria parasites
Malaria parasites are members of the genus
Plasmodium (phylum
Apicomplexa). In humans malaria is caused by
P. falciparum,
P. malariae,
P. ovale,
P. vivax and
P. knowlesi.[22][23]
P. falciparum is the most common cause of infection and is
responsible for about 80% of all malaria cases, and is also
responsible for about 90% of the deaths from malaria.[24]
Parasitic Plasmodium species also infect birds, reptiles,
monkeys, chimpanzees and rodents.[25]
There have been documented human infections with several
simian species of malaria, namely P. knowlesi,
P. inui,
P. cynomolgi,[26]
P. simiovale,
P. brazilianum,
P. schwetzi and
P. simium; however, with the exception of P. knowlesi,
these are mostly of limited public health importance.[27]
[edit]
Mosquito vectors and the Plasmodium life cycle
The parasite's primary (definitive)
hosts and transmission
vectors are female
mosquitoes of the
Anopheles genus, while humans and other vertebrates are
secondary hosts. Young mosquitoes first ingest the malaria parasite
by feeding on an infected human carrier and the infected
Anopheles mosquitoes carry Plasmodium
sporozoites in their
salivary glands.
A mosquito becomes infected when it takes a
blood meal from an infected human. Once ingested, the parasite
gametocytes taken up in the blood will further differentiate
into male or female
gametes and then fuse in the mosquito gut. This produces an
ookinete that penetrates the gut lining and produces an
oocyst in the gut wall. When the oocyst ruptures, it releases
sporozoites that migrate through the mosquito's body to the salivary
glands, where they are then ready to infect a new human host. This
type of transmission is occasionally referred to as anterior station
transfer.[28]
The sporozoites are injected into the skin, alongside saliva, when
the mosquito takes a subsequent blood meal.
Only female mosquitoes feed on blood, thus males do not transmit
the disease. The females of the Anopheles genus of mosquito
prefer to feed at night. They usually start searching for a meal at
dusk, and will continue throughout the night until taking a meal.
Malaria parasites can also be transmitted by
blood transfusions, although this is rare.[29]
[edit]
Pathogenesis

The life cycle of malaria parasites in the human body. A
mosquito infects a person by taking a blood meal. First,
sporozoites enter the bloodstream, and migrate to the
liver. They infect liver cells (hepatocytes), where they
multiply into merozoites, rupture the liver cells, and
escape back into the bloodstream. Then, the merozoites
infect red blood cells, where they develop into ring
forms, trophozoites and schizonts which in turn produce
further merozoites. Sexual forms (gametocytes) are also
produced, which, if taken up by a mosquito, will infect
the insect and continue the life cycle.
Malaria in humans develops via two phases: an exoerythrocytic and
an erythrocytic phase. The exoerythrocytic phase involves infection
of the hepatic system, or liver, whereas the erythrocytic phase
involves infection of the erythrocytes, or red blood cells. When an
infected mosquito pierces a person's skin to take a blood meal,
sporozoites in the mosquito's saliva enter the bloodstream and
migrate to the
liver.
Within 30 minutes of being introduced into the human host, the
sporozoites infect
hepatocytes, multiplying asexually and asymptomatically for a
period of 6–15 days. Once in the liver, these organisms
differentiate to yield thousands of
merozoites, which, following rupture of their host cells, escape
into the blood and infect
red blood cells, thus beginning the erythrocytic stage of the
life cycle.[30]
The parasite escapes from the liver undetected by wrapping itself in
the cell membrane of the infected host liver cell.[31]
Within the red blood cells, the parasites multiply further, again
asexually, periodically breaking out of their hosts to invade fresh
red blood cells. Several such amplification cycles occur. Thus,
classical descriptions of waves of fever arise from simultaneous
waves of merozoites escaping and infecting red blood cells.
Some P. vivax and P. ovale sporozoites do not
immediately develop into exoerythrocytic-phase merozoites, but
instead produce hypnozoites that remain dormant for periods ranging
from several months (6–12 months is typical) to as long as three
years. After a period of dormancy, they reactivate and produce
merozoites. Hypnozoites are responsible for long incubation and late
relapses in these two species of malaria.[32]
The parasite is relatively protected from attack by the body's
immune system because for most of its human life cycle it
resides within the liver and blood cells and is relatively invisible
to immune surveillance. However, circulating infected blood cells
are destroyed in the
spleen.
To avoid this fate, the P. falciparum parasite displays
adhesive
proteins on the surface of the infected blood cells, causing the
blood cells to stick to the walls of small blood vessels, thereby
sequestering the parasite from passage through the general
circulation and the spleen.[33]
This "stickiness" is the main factor giving rise to
hemorrhagic complications of malaria.
High endothelial venules (the smallest branches of the
circulatory system) can be blocked by the attachment of masses of
these infected red blood cells. The blockage of these vessels causes
symptoms such as in placental and cerebral malaria. In cerebral
malaria the sequestrated red blood cells can breach the
blood brain barrier possibly leading to coma.[34]
Although the red blood cell surface adhesive proteins (called
PfEMP1, for Plasmodium falciparum erythrocyte membrane
protein 1) are exposed to the immune system, they do not serve as
good immune targets, because of their extreme diversity; there are
at least 60 variations of the protein within a single parasite and
effectively limitless versions within parasite populations.[33]
The parasite switches between a broad repertoire of PfEMP1 surface
proteins, thus staying one step ahead of the pursuing immune system.
Some merozoites turn into male and female
gametocytes. If a mosquito pierces the skin of an infected
person, it potentially picks up gametocytes within the blood.
Fertilization and sexual recombination of the parasite occurs in the
mosquito's gut, thereby defining the mosquito as the
definitive host of the disease. New sporozoites develop and
travel to the mosquito's salivary gland, completing the cycle.
Pregnant women are especially attractive to the mosquitoes,[35]
and malaria in pregnant women is an important cause of
stillbirths, infant mortality and low birth weight,[36]
particularly in P. falciparum infection, but also in other
species infection, such as P. vivax.[37]
[edit]
Diagnosis

Blood smear from a
P. falciparum
culture (K1 strain). Several red blood cells have
ring stages inside them. Close to the center there is a
schizont and on the left a trophozoite.
Since Charles Laveran first visualised the malaria parasite in
blood in 1880,[38]
the mainstay of malaria diagnosis has been the microscopic
examination of blood.
Fever and septic shock are commonly misdiagnosed as severe
malaria in
Africa,
leading to a failure to treat other life-threatening illnesses. In
malaria-endemic areas,
parasitemia does not ensure a diagnosis of severe malaria,
because parasitemia can be incidental to other concurrent disease.
Recent investigations suggest that malarial
retinopathy is better (collective sensitivity of 95% and
specificity of 90%) than any other clinical or laboratory feature in
distinguishing malarial from non-malarial
coma.[39]
Although blood is the sample most frequently used to make a
diagnosis, both saliva and urine have been investigated as
alternative, less invasive specimens.[38]
[edit]
Symptomatic
diagnosis
Areas that cannot afford even simple laboratory diagnostic tests
often use only a history of subjective fever as the indication to
treat for malaria. Using Giemsa-stained blood smears from children
in Malawi, one study showed that when clinical predictors (rectal
temperature, nailbed pallor, and splenomegaly) were used as
treatment indications, rather than using only a history of
subjective fevers, a correct diagnosis increased from 21% to 41% of
cases, and unnecessary treatment for malaria was significantly
decreased.[40]
[edit]
Microscopic examination of blood films
The most economic, preferred, and reliable diagnosis of malaria
is microscopic examination of
blood films because each of the four major parasite species has
distinguishing characteristics. Two sorts of blood film are
traditionally used. Thin films are similar to usual blood films and
allow species identification because the parasite's appearance is
best preserved in this preparation. Thick films allow the
microscopist to screen a larger volume of blood and are about eleven
times more sensitive than the thin film, so picking up low levels of
infection is easier on the thick film, but the appearance of the
parasite is much more distorted and therefore distinguishing between
the different species can be much more difficult. With the pros and
cons of both thick and thin smears taken into consideration, it is
imperative to utilize both smears while attempting to make a
definitive diagnosis.[41]
From the thick film, an experienced microscopist can detect
parasite levels (or
parasitemia) down to as low as 0.0000001% of red blood cells.
Diagnosis of species can be difficult because the early trophozoites
("ring form") of all four species look identical and it is never
possible to diagnose species on the basis of a single ring form;
species identification is always based on several trophozoites.
One important thing to note is that P. malariae and P.
knowlesi (which is the most common cause of malaria in
South-east Asia) look very similar under the microscope.
However, P. knowlesi parasitemia increases very fast and
causes more severe disease than P. malariae, so it is
important to identify and treat infections quickly. Therefore modern
methods such as PCR (see "Molecular methods" below) or
monoclonal antibody panels that can distinguish between the two
should be used in this part of the world.
[42]
[edit]
Antigen tests
For areas where microscopy is not available, or where laboratory
staff are not experienced at malaria diagnosis, there are commercial
antigen detection tests that require only a drop of blood.[43]
Immunochromatographic tests (also called:
Malaria Rapid Diagnostic Tests, Antigen-Capture Assay or "Dipsticks")
been developed, distributed and fieldtested. These tests use
finger-stick or venous blood, the completed test takes a total of
15–20 minutes, and the results are read visually as the presence or
absence of colored stripes on the dipstick, so they are suitable for
use in the field. The threshold of detection by these rapid
diagnostic tests is in the range of 100 parasites/µl of blood
(commercial kits can range from about 0.002% to 0.1% parasitemia)
compared to 5 by thick film microscopy. One disadvantage is that
dipstick tests are qualitative but not quantitative - they can
determine if parasites are present in the blood, but not how many.
The first rapid diagnostic tests were using P. falciparum
glutamate dehydrogenase as antigen.[44]
PGluDH was soon replaced by P.falciparum
lactate dehydrogenase, a 33 kDa
oxidoreductase [EC 1.1.1.27]. It is the last enzyme of the
glycolytic pathway, essential for
ATP generation and one of the most abundant enzymes expressed by
P.falciparum. PLDH does not persist in the blood but clears
about the same time as the parasites following successful treatment.
The lack of antigen persistence after treatment makes the pLDH test
useful in predicting treatment failure. In this respect, pLDH is
similar to pGluDH. Depending on which
monoclonal antibodies are used, this type of assay can
distinguish between all five different species of human malaria
parasites, because of antigenic differences between their pLDH
isoenzymes.
[edit]
Molecular methods
Molecular methods are available in some clinical laboratories and
rapid real-time assays (for example,
QT-NASBA based on the
polymerase chain reaction)[45]
are being developed with the hope of being able to deploy them in
endemic areas.
PCR (and other molecular methods) is more accurate than
microscopy. However, it is expensive, and requires a specialized
laboratory. Moreover, levels of parasitemia are not necessarily
correlative with the progression of disease, particularly when the
parasite is able to adhere to blood vessel walls. Therefore more
sensitive, low-tech diagnosis tools need to be developed in order to
detect low levels of parasitemia in the field.
[46]
[edit]
Prevention

Anopheles albimanus mosquito feeding on a human
arm. This mosquito is a vector of malaria and mosquito
control is a very effective way of reducing the
incidence of malaria.
Methods used to prevent the spread of disease, or to protect
individuals in areas where malaria is endemic, include prophylactic
drugs, mosquito eradication, and the prevention of mosquito bites.
The continued existence of malaria in an area requires a combination
of high human population density, high mosquito population density,
and high rates of transmission from humans to mosquitoes and from
mosquitoes to humans. If any of these is lowered sufficiently, the
parasite will sooner or later disappear from that area, as happened
in
North America,
Europe
and much of
Middle East. However, unless the parasite is eliminated from the
whole world, it could become re-established if conditions revert to
a combination that favors the parasite's reproduction. Many
countries are seeing an increasing number of imported malaria cases
due to extensive travel and migration.
Many researchers argue that prevention of malaria may be more
cost-effective than treatment of the disease in the long run, but
the capital costs required are out of reach of many of the world's
poorest people. Economic adviser
Jeffrey Sachs estimates that malaria can be controlled for US$3
billion in aid per year.[47]
The distribution of funding varies among countries. Countries
with large populations do not receive the same amount of support.
The 34 countries that received a per capita annual support of less
than $1 included some of the poorest countries in Africa.
Brazil, Eritrea, India, and Vietnam have, unlike many other
developing nations, successfully reduced the malaria burden. Common
success factors included conducive country conditions, a targeted
technical approach using a package of effective tools, data-driven
decision-making, active leadership at all levels of government,
involvement of communities, decentralized implementation and control
of finances, skilled technical and managerial capacity at national
and sub-national levels, hands-on technical and programmatic support
from partner agencies, and sufficient and flexible financing.[48]
[edit]
Vector control
Efforts to
eradicate malaria by eliminating mosquitoes have been successful
in some areas. Malaria was once common in the
United States and southern
Europe,
but vector control programs, in conjunction with the monitoring and
treatment of infected humans, eliminated it from those regions. In
some areas, the draining of wetland breeding grounds and better
sanitation were adequate. Malaria was eliminated from the northern
parts of the USA in the early 20th century by such methods, and the
use of the
pesticide
DDT eliminated it from the South by 1951.[49]
In 2002, there were 1,059 cases of malaria reported in the US,
including eight deaths, but in only five of those cases was the
disease contracted in the United States.
Before DDT, malaria was successfully eradicated or controlled
also in several tropical areas by removing or poisoning the breeding
grounds of the mosquitoes or the aquatic habitats of the larva
stages, for example by filling or applying oil to places with
standing water. These methods have seen little application in Africa
for more than half a century.[50]
In the 1950s and 1960s, there was a major public health effort to
eradicate malaria worldwide by selectively targeting mosquitoes in
areas where malaria was rampant.[51]
However, these efforts have so far failed to eradicate malaria in
many parts of the developing world—the problem is most prevalent in
Africa.
Sterile insect technique is emerging as a potential mosquito
control method. Progress towards transgenic, or
genetically modified, insects suggest that wild mosquito
populations could be made malaria-resistant. Researchers at
Imperial College London created the world's first transgenic
malaria mosquito,[52]
with the first plasmodium-resistant species announced by a team at
Case Western Reserve University in
Ohio in
2002.[53]
Successful replacement of current populations with a new genetically
modified population, relies upon a drive mechanism, such as
transposable elements to allow for non-Mendelian inheritance of
the gene of interest. However, this approach contains many
difficulties and success is a distant prospect.[54]
An even more futuristic method of vector control is the idea that
lasers
could be used to kill flying mosquitoes.[55]
[edit]
Prophylactic drugs
Several drugs, most of which are also used for treatment of
malaria, can be taken preventively. Generally, these drugs are taken
daily or weekly, at a lower dose than would be used for treatment of
a person who had actually contracted the disease. Use of
prophylactic drugs is seldom practical for full-time residents of
malaria-endemic areas, and their use is usually restricted to
short-term visitors and travelers to malarial regions. This is due
to the cost of purchasing the drugs, negative
side effects from long-term use, and because some effective
anti-malarial drugs are difficult to obtain outside of wealthy
nations.
Quinine was used starting in the 17th century as a prophylactic
against malaria. The development of more effective alternatives such
as
quinacrine,
chloroquine, and
primaquine in the 20th century reduced the reliance on quinine.
Today, quinine is still used to treat chloroquine resistant
Plasmodium falciparum, as well as severe and cerebral stages
of malaria, but is not generally used for prophylaxis.
Modern drugs used preventively include
mefloquine (Lariam),
doxycycline (available generically), and the combination of
atovaquone and
proguanil hydrochloride (Malarone). The choice of which
drug to use depends on which drugs the parasites in the area are
resistant to, as well as side-effects and other considerations.
The prophylactic effect does not begin immediately upon starting
taking the drugs, so people temporarily visiting malaria-endemic
areas usually begin taking the drugs one to two weeks before
arriving and must continue taking them for 4 weeks after leaving
(with the exception of atovaquone proguanil that only needs be
started 2 days prior and continued for 7 days afterwards).
The use of prophylactic drugs where malaria-bearing mosquitoes
are present may encourage the development of partial immunity.[56]
[edit]
Indoor
residual spraying
Indoor residual spraying (IRS) is the practice of spraying
insecticides on the interior walls of homes in malaria affected
areas. After feeding, many mosquito species rest on a nearby surface
while digesting the bloodmeal, so if the walls of dwellings have
been coated with insecticides, the resting mosquitos will be killed
before they can bite another victim, transferring the malaria
parasite.
The first pesticide used for IRS was
DDT.[49]
Although it was initially used exclusively to combat malaria, its
use quickly spread to
agriculture. In time, pest-control, rather than disease-control,
came to dominate DDT use, and this large-scale agricultural use led
to the
evolution of resistant mosquitoes in many regions. The DDT
resistance shown by Anopheles mosquitoes can be compared to
antibiotic resistance shown by bacteria.
The overuse of
anti-bacterial soaps and antibiotics led to antibiotic resistance in
bacteria, similar to how overspraying of DDT on crops led to DDT
resistance in Anopheles mosquitoes. During the 1960s, awareness of
the negative consequences of its indiscriminate use increased,
ultimately leading to bans on agricultural applications of DDT in
many countries in the 1970s.
Since the use of DDT has been limited
or banned for agricultural use for some time, DDT may now be more
effective as a method of disease-control.
Although DDT has never been banned for use in malaria control and
there are several other insecticides suitable for IRS, some
advocates have claimed that bans are responsible for tens of
millions of deaths in tropical countries where DDT had once been
effective in controlling malaria. Furthermore, most of the problems
associated with DDT use stem specifically from its industrial-scale
application in agriculture, rather than its use in
public health.[57]
The
World Health Organization (WHO) currently advises the use of 12
different insecticides in IRS operations. These include DDT and a
series of alternative insecticides (such as the pyrethroids
permethrin and
deltamethrin), to combat malaria in areas where mosquitoes are
DDT-resistant and to slow the evolution of resistance.[58]
This public health use of small amounts of DDT is permitted under
the
Stockholm Convention on
Persistent Organic Pollutants (POPs), which prohibits the
agricultural use of DDT.[59]
However, because of its legacy, many developed countries discourage
DDT use even in small quantities.[60][61]
One problem with all forms of Indoor Residual Spraying is
insecticide
resistance via evolution of mosquitos. According to a study
published on Mosquito Behavior and Vector Control, mosquito species
that are affected by IRS are endophilic species (species that tend
to rest and live indoors), and due to the irritation caused by
spraying, their evolutionary descendants are trending towards
becoming exophilic (species that tend to rest and live out of
doors), meaning that they are not as affected—if affected at all—by
the IRS, rendering it somewhat useless as a defense mechanism.[62]
[edit]
Mosquito
nets and bedclothes
Main article:
Mosquito netMosquito nets help keep mosquitoes away from people and greatly
reduce the infection and transmission of malaria. The nets are not a
perfect barrier and they are often treated with an insecticide
designed to kill the mosquito before it has time to search for a way
past the net. Insecticide-treated nets (ITNs) are estimated to be
twice as effective as untreated nets and offer greater than 70%
protection compared with no net.[63]
Although ITNs are proven to be very effective against malaria, less
than 2% of children in urban areas in Sub-Saharan Africa are
protected by ITNs. Since the
Anopheles mosquitoes feed at night, the preferred method is
to hang a large "bed net" above the center of a bed such that it
drapes down and covers the bed completely.
The distribution of mosquito nets impregnated with insecticides
such as
permethrin or deltamethrin has been shown to be an extremely
effective method of malaria prevention, and it is also one of the
most cost-effective methods of prevention. These nets can often be
obtained for around
US$2.50 to US$3.50 (€2
to €3) from the
United Nations, the World Health Organization (WHO), and others.
ITNs have been shown to be the most cost-effective prevention method
against malaria and are part of WHO’s Millennium Development Goals
(MDGs).
While some experts argue that international organizations should
distribute ITNs and LLINs to people for free in order to maximize
coverage (since such a policy would reduce price barriers), others
insist that cost-sharing between the international organization and
recipients would lead to greater usage of the net (arguing that
people will value a net more if they pay for it). Additionally,
proponents of cost-sharing argue that such a policy ensures that
nets are efficiently allocated to those people who most need them
(or are most vulnerable to infection). Through a "selection effect",
they argue, those people who most need the bed nets will choose to
purchase them, while those less in need will opt out.
However, a randomized controlled trial study of ITNs uptake among
pregnant women in Kenya, conducted by economists Pascaline Dupas and
Jessica Cohen, found that cost-sharing does not necessarily increase
the usage intensity of ITNs, nor does it induce uptake by those most
vulnerable to infection, as compared to a policy of free
distribution.[64]
In some cases, cost-sharing can actually decrease demand for
mosquito nets by erecting a price barrier. Dupas and Cohen’s
findings support the argument that free distribution of ITNs can be
more effective than cost-sharing in both increasing coverage and
saving lives. In a cost-effectiveness analysis, Dupas and Cohen note
that "cost-sharing is at best marginally more cost-effective than
free distribution, but free distribution leads to many more lives
saved."[64]
The researchers base their conclusions about the
cost-effectiveness of free distribution on the proven spillover
benefits of increased ITN usage.[65]
When a large number of nets are distributed in one residential area,
their chemical additives help reduce the number of mosquitoes in the
environment. With fewer mosquitoes in the environment, the chances
of malaria infection for recipients and non-recipients are
significantly reduced. (In other words, the importance of the
physical barrier effect of ITNs decreases relative to the positive
externality effect of the nets in creating a mosquito-free
environment when ITNs are highly concentrated in one residential
cluster or community.)
For maximum effectiveness, the nets should be re-impregnated with
insecticide every six months. This process poses a significant
logistical problem in rural areas. New technologies like Olyset or
DawaPlus allow for production of long-lasting insecticidal mosquito
nets (LLINs), which release insecticide for approximately 5 years,[66]
and cost about US$5.50. ITNs protect people sleeping under the net
and simultaneously kill mosquitoes that contact the net. Some
protection is also provided to others by this method, including
people sleeping in the same room but not under the net.
While distributing mosquito nets is a major component of malaria
prevention, community education and awareness on the dangers of
malaria are associated with distribution campaigns to make sure
people who receive a net know how to use it. "Hang Up" campaigns,
such as the ones conducted by volunteers of the
International Red Cross and Red Crescent Movement consist of
visiting households that received a net at the end of the campaign
or just before the rainy season, ensuring that the net is being used
properly and that the people most vulnerable to malaria, such as
young children and the elderly, sleep under it. A study conducted by
the
CDC in
Sierra Leone showed a 22 percent increase in net utilization
following a personal visit from a volunteer living in the same
community promoting net usage. A study in
Togo
showed similar improvements.[67]
Mosquito nets are often unaffordable to people in developing
countries, especially for those most at risk. Only 1 out of 20
people in Africa own a bed net. Nets are also often distributed
though vaccine campaigns using voucher subsidies, such as the
measles campaign for children. A study among
Afghan refugees in Pakistan found that treating top-sheets and
chaddars (head coverings) with permethrin has similar effectiveness
to using a treated net, but is much cheaper.[68]
Another alternative approach uses spores of the
fungus
Beauveria bassiana, sprayed on walls and bed nets, to kill
mosquitoes. While some mosquitoes have developed resistance to
chemicals, they have not been found to develop a resistance to
fungal infections.[69]
[edit]
Vaccination
Immunity (or, more accurately, tolerance) does occur naturally,
but only in response to repeated infection with multiple strains of
malaria.[70]
Vaccines for malaria are under development, with no completely
effective vaccine yet available. The first promising studies
demonstrating the potential for a malaria vaccine were performed in
1967 by immunizing mice with live, radiation-attenuated
sporozoites, providing protection to about 60% of the mice upon
subsequent injection with normal, viable sporozoites.[71]
Since the 1970s, there has been a considerable effort to develop
similar vaccination strategies within humans. It was determined that
an individual can be protected from a P. falciparum infection
if they receive over 1,000 bites from infected, irradiated
mosquitoes.[72]
It has been generally accepted that it is impractical to provide
at-risk individuals with this vaccination strategy, but that has
been recently challenged with work being done by Dr. Stephen
Hoffman, one of the key researchers who originally sequenced the
genome of
Plasmodium falciparum. His work most recently has revolved
around solving the logistical problem of isolating and preparing the
parasites equivalent to 1000 irradiated mosquitoes for mass storage
and inoculation of human beings. The company has recently received
several multi-million dollar grants from the
Bill & Melinda Gates Foundation and the U.S. government to begin
early clinical studies in 2007 and 2008.[73]
The Seattle Biomedical Research Institute (SBRI), funded by the
Malaria Vaccine Initiative, assures potential volunteers that "the
[2009] clinical trials won't be a life-threatening experience. While
many volunteers [in Seattle] will actually contract malaria, the
cloned strain used in the experiments can be quickly cured, and does
not cause a recurring form of the disease. Some participants will
get experimental drugs or vaccines, while others will get placebo."[74]
Instead, much work has been performed to try and understand the
immunological processes that provide protection after
immunization with irradiated sporozoites. After the mouse
vaccination study in 1967,[71]
it was hypothesized that the injected sporozoites themselves were
being recognized by the immune system, which was in turn creating
antibodies against the parasite. It was determined that the
immune system was creating antibodies against the
circumsporozoite protein (CSP) which coated the sporozoite.[75]
Moreover, antibodies against CSP prevented the sporozoite from
invading hepatocytes.[76]
CSP was therefore chosen as the most promising protein on which to
develop a vaccine against the malaria sporozoite. It is for these
historical reasons that vaccines based on CSP are the most numerous
of all malaria vaccines.
Presently, there is a huge variety of vaccine candidates on the
table. Pre-erythrocytic vaccines (vaccines that target the parasite
before it reaches the blood), in particular vaccines based on CSP,
make up the largest group of research for the malaria vaccine. There
have been recent breakthroughs in vaccines that seek to avoid more
severe pathologies of malaria by preventing adherence of the
parasite to blood
venules and
placenta, but financing is not yet in place for trials.[77]
Other potential vaccines include those that seek to induce immunity
to the blood stages of the infection and
transmission-blocking vaccines that would stop the development
of the parasite in the mosquito right after the mosquito has taken a
bloodmeal from an infected person.[78]
It is hoped that the knowledge of the P. falciparum
genome,
the sequencing of which was completed in 2002,[79]
will provide targets for new drugs or vaccines.[80]
The first vaccine developed that has undergone field trials, is
the SPf66, developed by
Manuel Elkin Patarroyo in 1987. It presents a combination of
antigens from the sporozoite (using CS repeats) and merozoite
parasites. During phase I trials a 75% efficacy rate was
demonstrated and the vaccine appeared to be well tolerated by
subjects and immunogenic. The phase IIb and III trials were less
promising, with the efficacy falling to between 38.8% and 60.2%. A
trial was carried out in Tanzania in 1993 demonstrating the efficacy
to be 31% after a years follow up, however the most recent (though
controversial) study in The Gambia did not show any effect. Despite
the relatively long trial periods and the number of studies carried
out, it is still not known how the SPf66 vaccine confers immunity;
it therefore remains an unlikely solution to malaria. The CSP was
the next vaccine developed that initially appeared promising enough
to undergo trials. It is also based on the circumsporoziote protein,
but additionally has the recombinant
(Asn-Ala-Pro15Asn-Val-Asp-Pro)2-Leu-Arg(R32LR) protein covalently
bound to a purified
Pseudomonas aeruginosa toxin (A9). However at an early stage
a complete lack of protective immunity was demonstrated in those
inoculated. The study group used in Kenya had an 82% incidence of
parasitaemia whilst the control group only had an 89% incidence. The
vaccine intended to cause an increased T-lymphocyte response in
those exposed, this was also not observed.
The efficacy of Patarroyo's vaccine has been disputed with some
US scientists concluding in
The Lancet (1997) that "the vaccine was not effective and should
be dropped" while the Colombian accused them of "arrogance" putting
down their assertions to the fact that he came from a developing
country.
The RTS,S/AS02A vaccine is the candidate furthest along in
vaccine trials. It is being developed by a partnership between the
PATH Malaria Vaccine Initiative (a grantee of the
Gates Foundation), the
pharmaceutical company,
GlaxoSmithKline, and the
Walter Reed Army Institute of Research.[81]
In the vaccine, a portion of CSP has been fused to the
immunogenic "S
antigen" of the
hepatitis B virus; this
recombinant protein is injected alongside the potent AS02A
adjuvant.[78]
In October 2004, the RTS,S/AS02A researchers announced results of a
Phase IIb trial, indicating the vaccine reduced infection risk
by approximately 30% and severity of infection by over 50%. The
study looked at over 2,000
Mozambican children.[82]
More recent testing of the RTS,S/AS02A vaccine has focused on the
safety and efficacy of administering it earlier in infancy: In
October 2007, the researchers announced results of a
phase I/IIb trial conducted on 214 Mozambican infants between
the ages of 10 and 18 months in which the full three-dose course of
the vaccine led to a 62% reduction of infection with no serious
side-effects save some pain at the point of injection.[83]
Further research will delay this vaccine from commercial release
until around 2011.[84]
On 6 April 2010,
Crucell, a Dutch biopharmaceutical company, has signed a binding
letter of agreement with
GlaxoSmithKline Biologicals (GSK) to collaborate on developing
malaria vaccine candidate.
[edit]
Other methods
Education in recognizing the symptoms of malaria has reduced the
number of cases in some areas of the developing world by as much as
20%. Recognizing the disease in the early stages can also stop the
disease from becoming a killer. Education can also inform people to
cover over areas of stagnant, still water e.g. Water Tanks which are
ideal breeding grounds for the parasite and mosquito, thus cutting
down the risk of the transmission between people. This is most put
in practice in urban areas where there are large centers of
population in a confined space and transmission would be most likely
in these areas.
The
Malaria Control Project is currently using downtime computing
power donated by individual volunteers around the world (see
Volunteer computing and
BOINC) to simulate models of the health effects and transmission
dynamics in order to find the best method or combination of methods
for malaria control. This modeling is extremely computer intensive
due to the simulations of large human populations with a vast range
of parameters related to biological and social factors that
influence the spread of the disease. It is expected to take a few
months using volunteered computing power compared to the 40 years it
would have taken with the current resources available to the
scientists who developed the program.[85]
An example of the importance of computer modeling in planning
malaria
eradication programs is shown in the paper by Águas and others.
They showed that eradication of malaria is crucially dependent on
finding and treating the large number of people in endemic areas
with asymptomatic malaria, who act as a reservoir for infection.[86]
The malaria parasites do not affect animal species and therefore
eradication of the disease from the human population would be
expected to be effective.
Other interventions for the control of malaria include
mass drug administrations and
intermittent preventive therapy.
Another was of reducing the malaria transmited to humans from
mosquitoes has been developed by the University of Arizona. They
have engenered a mosquito to become resistent to malaria. This was
reported on the 16 July 2010 in the journal
PLoS Pathogens.[87]
With the ultimate end being that the release of this GM mosquito
into the environment, Gareth Lycett, a malaria researcher from
Liverpool School of Tropical Medicine told the BBC that "It is
another step on the journey towards potentially assisting malaria
control through GM mosquito release."[88]
[edit]
Treatment
Active malaria infection with P. falciparum is a
medical emergency requiring
hospitalization. Infection with P. vivax, P. ovale
or P. malariae can often be treated on an outpatient basis.
Treatment of malaria involves supportive measures as well as
specific
antimalarial drugs. Most antimalarial drugs are produced
industrially and are sold at pharmacies.
However, as the cost of
such medicines are often too high for most people in the developing
world, some herbal remedies (such as Artemisia annua tea[89])
have also been developed, and have gained support from international
organisations such as
Médicins Sans Frontières. When properly treated, someone with
malaria can expect a complete recovery.[90]
[edit]
Counterfeit drugs
Sophisticated
counterfeits have been found in several Asian countries such as
Cambodia,[91]
China,[92]
Indonesia,
Laos,
Thailand,
Vietnam and are an important cause of avoidable death in those
countries.[93]
WHO have said that studies indicate that up to 40% of
artesunate based malaria medications are counterfeit, especially
in the Greater
Mekong
region and have established a rapid alert system to enable
information about counterfeit drugs to be rapidly reported to the
relevant authorities in participating countries.[94]
There is no reliable way for doctors or lay people to detect
counterfeit drugs without help from a laboratory. Companies are
attempting to combat the persistence of counterfeit drugs by using
new technology to provide security from source to distribution.
[edit]
Epidemiology

Countries which have regions where malaria is
endemic as of 2003 (coloured yellow).
[95]
Countries in green are free of indigenous cases of
malaria in all areas.
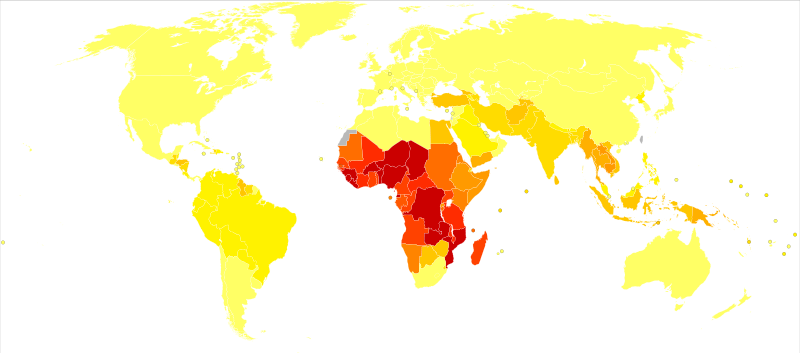
Disability-adjusted life year for malaria per
100,000 inhabitants in 2002.
no data =10
10-50 50-100
100-250 250-500
500-1000 1000-1500
1500-2000 2000-2500
2500-3000 3000-3500
=3500
Malaria causes about 250 million cases of fever and approximately
one million deaths annually.[96]
The vast majority of cases occur in children under 5 years old;[97]
pregnant women are also especially vulnerable. Despite efforts to
reduce transmission and increase treatment, there has been little
change in which areas are at risk of this disease since 1992.[98]
Indeed, if the prevalence of malaria stays on its present upwards
course, the death rate could double in the next twenty years.[99]
Precise statistics are unknown because many cases occur in rural
areas where people do not have access to hospitals or the means to
afford health care. As a consequence, the majority of cases are
undocumented.[99]
Although co-infection with HIV and malaria does cause increased
mortality, this is less of a problem than with HIV/tuberculosis
co-infection, due to the two diseases usually attacking different
age-ranges, with malaria being most common in the young and active
tuberculosis most common in the old.[100]
Although HIV/malaria co-infection produces less severe symptoms than
the interaction between HIV and TB, HIV and malaria do contribute to
each other's spread. This effect comes from malaria increasing
viral load and HIV infection increasing a person's
susceptibility to malaria infection.[101]
Malaria is presently endemic in a broad band around the equator,
in areas of the
Americas, many parts of
Asia,
and much of
Africa;
however, it is in sub-Saharan Africa where 85– 90% of malaria
fatalities occur.[102]
The geographic distribution of malaria within large regions is
complex, and malaria-afflicted and malaria-free areas are often
found close to each other.[103]
In drier areas, outbreaks of malaria can be predicted with
reasonable accuracy by mapping rainfall.[104]
Malaria is more common in rural areas than in cities; this is in
contrast to
dengue fever where urban areas present the greater risk.[105]
For example, the cities of
Vietnam,
Laos
and
Cambodia are essentially malaria-free, but the disease is
present in many rural regions.[106]
By contrast, in Africa malaria is present in both rural and urban
areas, though the risk is lower in the larger cities.[107]
The global
endemic levels of malaria have not been mapped since the 1960s.
However, the
Wellcome Trust, UK, has funded the
Malaria Atlas Project[108]
to rectify this, providing a more contemporary and robust means with
which to assess current and future malaria
disease burden.
[edit]
History
Malaria has infected humans for over 50,000 years, and
Plasmodium may have been a human
pathogen for the entire history of the species.[109]
Close relatives of the human malaria parasites remain common in
chimpanzees.[110]
References to the unique periodic fevers of malaria are found
throughout recorded history, beginning in 2700 BC in China.[111]
Malaria may have contributed to the decline of the
Roman Empire,[112]
and was so pervasive in Rome that it was known as the "Roman
fever".[113]
The term malaria originates from
Medieval
Italian: mala aria — "bad
air"; the disease was formerly called ague or marsh
fever due to its association with swamps and marshland.[114]
Malaria was once common in most of
Europe
and
North America,[115]
where it is no longer
endemic,[116]
though imported cases do occur.
Malaria was the most important
health hazard encountered by U.S. troops in the South Pacific during
World War II, where about 500,000 men were infected.[117]
Sixty thousand American soldiers died of malaria during the North
African and South Pacific campaigns.[118]
Scientific studies on malaria made their first significant
advance in 1880, when a French army doctor working in the military
hospital of
Constantine in
Algeria named
Charles Louis Alphonse Laveran observed parasites for the first
time, inside the
red blood cells of people suffering from malaria. He, therefore,
proposed that malaria is caused by this organism, the first time a
protist was identified as causing disease.[119]
For this and later discoveries, he was awarded the 1907
Nobel Prize for Physiology or Medicine.
The malarial parasite
was called Plasmodium by the Italian scientists
Ettore Marchiafava and
Angelo Celli.[120]
A year later,
Carlos Finlay, a Cuban doctor treating patients with
yellow fever in
Havana,
provided strong evidence that mosquitoes were transmitting disease
to and from humans.[121]
This work followed earlier suggestions by
Josiah C. Nott,[122]
and work by
Patrick Manson on the transmission of
filariasis.[123]
It was Britain's
Sir Ronald Ross, working in the
Presidency General Hospital in
Calcutta, who finally proved in 1898 that malaria is transmitted
by mosquitoes. He did this by showing that certain mosquito species
transmit malaria to birds. He isolated malaria parasites from the
salivary glands of mosquitoes that had fed on infected birds.[124]
For this work, Ross received the 1902 Nobel Prize in Medicine.
After
resigning from the Indian Medical Service, Ross worked at the newly
established
Liverpool School of Tropical Medicine and directed
malaria-control efforts in
Egypt,
Panama,
Greece
and
Mauritius.[125]
The findings of Finlay and Ross were later confirmed by a medical
board headed by
Walter Reed in 1900. Its recommendations were implemented by
William C. Gorgas in
the health measures undertaken during construction of the
Panama Canal. This public-health work saved the lives of
thousands of workers and helped develop the methods used in future
public-health campaigns against the disease.
The first effective treatment for malaria came from the bark of
cinchona tree, which contains
quinine. This tree grows on the slopes of the
Andes,
mainly in
Peru. The
indigenous peoples of Peru made a tincture of cinchona to
control malaria. The
Jesuits noted the efficacy of the practice and introduced the
treatment to Europe during the 1640s, where it was rapidly accepted.[126]
It was not until 1820 that the active ingredient, quinine, was
extracted from the bark, isolated and named by the French chemists
Pierre Joseph Pelletier and
Joseph Bienaimé Caventou.[127]
In the early 20th century, before
antibiotics became available,
Julius Wagner-Jauregg discovered that patients with
syphilis could be treated by intentionally infecting them with
malaria; the resulting fever would kill the syphilis
spirochetes, and
quinine could be administered to control the malaria. Although
some patients died from malaria, this was considered preferable to
the almost-certain death from syphilis.[128]
The first successful continuous
malaria culture was established in 1976 by William Trager and
James B. Jensen, which facilitated research into the molecular
biology of the parasite and the development of new drugs.[129][130]
Although the blood stage and mosquito stages of the malaria life
cycle were identified in the 19th and early 20th centuries, it was
not until the 1980s that the latent liver form of the parasite was
observed.[131][132]
The discovery of this latent form of the parasite explained why
people could appear to be cured of malaria but suffer relapse years
after the parasite had disappeared from their bloodstreams.
[edit]
Genetic
resistance to malaria
Malaria is thought to have been the greatest
selective pressure on the
human genome in recent history.[133]
This is due to the high levels of
mortality
and
morbidity caused by malaria, especially the
P. falciparum species.
[edit]
Sickle-cell
disease

Frequency and origin of malaria cases in 1996.
[134]
? High Risk
? Medium Risk
? Low Risk
? Very Low
Risk
? No Risk
The most-studied influence of the malaria parasite upon the human
genome is a hereditary blood disease,
sickle-cell disease. The sickle-cell trait causes disease, but
even those only partially affected by sickle-cell have substantial
protection against malaria.
In sickle-cell disease, there is a mutation in the HBB
gene, which encodes the beta-globin subunit of
haemoglobin. The normal allele encodes a
glutamate at position six of the beta-globin protein, whereas
the sickle-cell allele encodes a
valine.
This change from a hydrophilic to a hydrophobic amino acid
encourages binding between haemoglobin molecules, with
polymerization of haemoglobin deforming red blood cells into a
"sickle" shape. Such deformed cells are cleared rapidly from the
blood, mainly in the spleen, for destruction and recycling.
In the merozoite stage of its life cycle, the malaria parasite
lives inside red blood cells, and its metabolism changes the
internal chemistry of the red blood cell. Infected cells normally
survive until the parasite reproduces, but, if the red cell contains
a mixture of sickle and normal haemoglobin, it is likely to become
deformed and be destroyed before the daughter parasites emerge.
Thus, individuals
heterozygous for the mutated allele, known as sickle-cell trait,
may have a low and usually unimportant level of
anaemia, but also have a greatly reduced chance of serious
malaria infection. This is a classic example of
heterozygote advantage.
Individuals
homozygous for the mutation have full sickle-cell disease and in
traditional societies rarely live beyond adolescence. However, in
populations where malaria is
endemic, the
frequency of sickle-cell genes is around 10%. The existence of
four
haplotypes of sickle-type hemoglobin suggests that this mutation
has emerged
independently at least four times in malaria-endemic areas,
further demonstrating its evolutionary advantage in such affected
regions. There are also other mutations of the HBB gene that produce
haemoglobin molecules capable of conferring similar resistance to
malaria infection. These mutations produce haemoglobin types HbE and
HbC, which are common in
Southeast Asia and
Western Africa, respectively.
[edit]
Thalassaemias
Another well-documented set of mutations found in the human
genome associated with malaria are those involved in causing blood
disorders known as
thalassaemias. Studies in
Sardinia and
Papua New Guinea have found that the
gene frequency of
ß-thalassaemias is related to the level of malarial endemicity
in a given population. A study on more than 500 children in
Liberia found that those with ß-thalassaemia had a 50% decreased
chance of getting clinical malaria. Similar studies have found links
between gene frequency and malaria endemicity in the a+ form of a-thalassaemia.
Presumably these genes have also been
selected in the course of human evolution.
[edit]
Duffy antigens
The
Duffy antigens are
antigens expressed on red blood cells and other cells in the
body acting as a
chemokine receptor. The expression of Duffy antigens on blood
cells is encoded by Fy genes (Fya, Fyb, Fyc etc.).
Plasmodium vivax malaria uses the Duffy antigen to enter
blood cells. However, it is possible to express no Duffy antigen on
red blood cells (Fy-/Fy-). This
genotype confers complete resistance to P. vivax
infection. The genotype is very rare in European, Asian and American
populations, but is found in almost all of the indigenous population
of West and Central Africa.[135]
This is thought to be due to very high exposure to P. vivax
in
Africa in the last few thousand years.
Glucose-6-phosphate dehydrogenase (G6PD) is an
enzyme
that normally protects from the effects of
oxidative stress in red blood cells. However, a genetic
deficiency in this enzyme results in increased protection against
severe malaria.
[edit]
HLA and
interleukin-4
HLA-B53 is associated with low risk of severe malaria. This
MHC class I molecule presents
liver
stage and
sporozoite
antigens to
T-Cells. Interleukin-4, encoded by IL4, is produced by activated
T cells and promotes proliferation and differentiation of
antibody-producing B cells. A study of the Fulani of Burkina Faso,
who have both fewer malaria attacks and higher levels of
antimalarial antibodies than do neighboring ethnic groups, found
that the IL4-524 T allele was associated with elevated antibody
levels against malaria antigens, which raises the possibility that
this might be a factor in increased resistance to malaria.[136]
[edit]
Resistance
in South Asia
The lowest Himalayan Foothills and
Inner Terai or Doon Valleys of
Nepal
and India
are highly malarial due to a warm climate and marshes sustained
during the dry season by groundwater percolating down from the
higher hills. Malarial forests were intentionally maintained by the
rulers of Nepal as a defensive measure. Humans attempting to live in
this zone suffered much higher mortality than at higher elevations
or below on the drier
Gangetic Plain.
However, the
Tharu people had lived in this zone long enough to evolve
resistance via multiple genes. Medical studies among the Tharu and
non-Tharu population of the
Terai
yielded the evidence that the prevalence of cases of residual
malaria is nearly seven times lower among Tharus. The basis for
their resistance to malaria is most likely a genetic factor.
Endogamy along caste and ethnic lines appear to have confined
these to the Tharu community.[137]
Otherwise these genes probably would have become nearly universal in
South Asia and beyond because of their considerable survival value
and the apparent lack of negative effects comparable to Sickle Cell
Anemia.
[edit]
Society and
culture
Malaria is not just a disease commonly associated with poverty
but also a cause of poverty and a major hindrance to
economic development. Tropical regions are affected most,
however malaria’s furthest extent reaches into some temperate zones
with extreme seasonal changes. The disease has been associated with
major negative economic effects on regions where it is widespread.
During the late 19th and early 20th centuries, it was a major factor
in the slow economic development of the American southern states.[138].
A comparison of average per capita GDP in 1995, adjusted for
parity of purchasing power, between countries with malaria and
countries without malaria gives a fivefold difference ($1,526 USD
versus $8,268 USD). In countries where malaria is common, average
per capita GDP has risen (between 1965 and 1990) only 0.4% per year,
compared to 2.4% per year in other countries.[139]
Poverty is both cause and effect, however, since the poor do not
have the financial capacities to prevent or treat the disease. The
lowest income group in Malawi carries (1994) the burden of having
32% of their annual income used on this disease compared with the 4%
of household incomes from low-to-high groups.[140]
In its entirety, the economic impact of malaria has been estimated
to cost Africa $12 billion USD every year. The economic impact
includes costs of health care, working days lost due to sickness,
days lost in education, decreased productivity due to brain damage
from cerebral malaria, and loss of investment and tourism.[97]
In some countries with a heavy malaria burden, the disease may
account for as much as 40% of public health expenditure, 30-50% of
inpatient admissions, and up to 50% of outpatient visits.[141]
[edit]
See also
























